la Science aveuglée par la passion
par Isabelle Bourdial
CE QUE DISENT
LES ANALYSES MÉDICO-CHIRURGICALES
De nombreux médecins ont pratiqué l'analyse médico-chirurgicale et biologique du suaire. Ils ont recensé plusieurs plaies sanglantes ou semblant telles. Elles prédominent sur la partie droite du visage, qui semble tuméfiée. Le nez paraît fracturé. Des saignements en coulées, supposés provenir des piqûres d'épines de la couronne, sont visibles sur le front et le cuir chevelu.
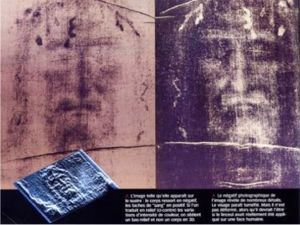
L'image telle qu'elle apparaît sur le suaire: le corps ressort en négatif, les taches de « sang » en positif. Si l'on traduit en relief (ci-contre) les variations d'intensité de couleur, on obtient un bas-relief
et non un corps en 3D.
Le négatif photographique de l'image révèle de nombreux détails. Le visage paraît tuméfié. Mais il n'est pas déformé, alors qu'il devrait l'être si le linceul avait réellement été appliqué sur une face humaine.
Les lésions du corps évoquent la flagellation. Le nombre d'impacts recensés est de 100 à 120. De légères écorchures s'étendent sur une surface de 9 cm sur 10 sur le trajet possible du frottement produit par l'angle entre le stipes (l'axe vertical de la croix) et le patibulum (son axe horizontal). Les genoux sont écorchés.
Une plaie est visible au côté droit, de 4 cm par 1,5 cm, taille compatible avec la pointe de la lancea romaine de l'époque, en tenant compte de la rétraction post mortem des chairs. Elle est située au niveau du cinquième espace intercostal. En est issu un liquide évoquant du sang épais, s'écoulant verticalement, modelé sur le muscle grand dentelé. Il peut correspondre à un écoulement abondant d'eau et de sang provenant soit d'un épanchement pleural, soit d'un hydropéricarde pré-agonique ou post-traumatique (c'est-à-dire la présence de liquide dans la membrane qui entoure le cur). Une deuxième coulée, postérieure et transversale, pourrait s'expliquer par l'horizontalisation du corps après la descente de la croix et la vidange de la veine cave inférieure contenant le sang du retour veineux.
Par ailleurs, le thorax est distendu, le creux épigastrique affaissé, l'abdomen proéminent, les quadriceps et les fessiers saillants, autant de signes de l'asphyxie provoquée par la position des bras inclinés à 65° par rapport au stipes. Car lors d'une crucifixion, la cage thoracique ne peut plus s'expandre, l'oxygène se raréfie, le gaz carbonique et les lactates, produits du métabolisme anaérobie, s'accumulent, causant une acidose respiratoire et métabolique et une tétanisation des muscles. Au début, l'appui sur les pieds permet de redresser le corps et facilite l'inspiration. Mais surviennent bientôt la détresse respiratoire et la défaillance cardio-circulatoire conduisant à la mort. Toutefois, certains médecins tels Frederick Zugibe, pensent que la crucifixion ne provoque pas d'asphyxie (voir p. 124).
Selon le Dr Véronique di Costanzo-Etienne de l'hôpital de Toulon, les caractéristiques de toutes ces lésions répondent à des impératifs anatomiques difficiles à contrefaire sans connaissances médicales. Tel n'est pas l'avis du Pr Claude Got, anatomo-pathologiste expert du Conseil national de la sécurité routière, pour qui cette analyse est un mélange de description et d'interprétation. Pour lui, la démarche ne se borne pas à décrire la totalité des faits visibles. Elle s'apparente à une recherche d'explication a posteriori qui tente, consciemment ou non de coller à la passion du Christ. « L'imprécision du contour de ces empreintes ne me permet pas d'avancer une interprétation physiopathologique. Rien dans leur forme et leur couleur ne me dit que ces taches sont de nature biologique » conclut-il.
L'image telle qu'elle apparaît sur le suaire: le corps ressort en négatif, les taches de « sang » en positif. Si l'on traduit en relief (ci-contre) les variations d'intensité de couleur, on obtient un bas-relief
et non un corps en 3D.
Le négatif photographique de l'image révèle de nombreux détails. Le visage paraît tuméfié. Mais il n'est pas déformé, alors qu'il devrait l'être si le linceul avait réellement été appliqué sur une face humaine.
Les lésions du corps évoquent la flagellation. Le nombre d'impacts recensés est de 100 à 120. De légères écorchures s'étendent sur une surface de 9 cm sur 10 sur le trajet possible du frottement produit par l'angle entre le stipes (l'axe vertical de la croix) et le patibulum (son axe horizontal). Les genoux sont écorchés.
Une plaie est visible au côté droit, de 4 cm par 1,5 cm, taille compatible avec la pointe de la lancea romaine de l'époque, en tenant compte de la rétraction post mortem des chairs. Elle est située au niveau du cinquième espace intercostal. En est issu un liquide évoquant du sang épais, s'écoulant verticalement, modelé sur le muscle grand dentelé. Il peut correspondre à un écoulement abondant d'eau et de sang provenant soit d'un épanchement pleural, soit d'un hydropéricarde pré-agonique ou post-traumatique (c'est-à-dire la présence de liquide dans la membrane qui entoure le cur). Une deuxième coulée, postérieure et transversale, pourrait s'expliquer par l'horizontalisation du corps après la descente de la croix et la vidange de la veine cave inférieure contenant le sang du retour veineux.
Par ailleurs, le thorax est distendu, le creux épigastrique affaissé, l'abdomen proéminent, les quadriceps et les fessiers saillants, autant de signes de l'asphyxie provoquée par la position des bras inclinés à 65° par rapport au stipes. Car lors d'une crucifixion, la cage thoracique ne peut plus s'expandre, l'oxygène se raréfie, le gaz carbonique et les lactates, produits du métabolisme anaérobie, s'accumulent, causant une acidose respiratoire et métabolique et une tétanisation des muscles. Au début, l'appui sur les pieds permet de redresser le corps et facilite l'inspiration. Mais surviennent bientôt la détresse respiratoire et la défaillance cardio-circulatoire conduisant à la mort. Toutefois, certains médecins tels Frederick Zugibe, pensent que la crucifixion ne provoque pas d'asphyxie (voir p. 124).
Selon le Dr Véronique di Costanzo-Etienne de l'hôpital de Toulon, les caractéristiques de toutes ces lésions répondent à des impératifs anatomiques difficiles à contrefaire sans connaissances médicales. Tel n'est pas l'avis du Pr Claude Got, anatomo-pathologiste expert du Conseil national de la sécurité routière, pour qui cette analyse est un mélange de description et d'interprétation. Pour lui, la démarche ne se borne pas à décrire la totalité des faits visibles. Elle s'apparente à une recherche d'explication a posteriori qui tente, consciemment ou non de coller à la passion du Christ. « L'imprécision du contour de ces empreintes ne me permet pas d'avancer une interprétation physiopathologique. Rien dans leur forme et leur couleur ne me dit que ces taches sont de nature biologique » conclut-il.
Science blinded with passion
by Isabelle Bourdial
THE RESULTS OF
THE MEDICO-SURGICAL ANALYSES
Several doctors carried out the medico-surgical and biological analysis of the shroud. They listed several wounds bloody or seeming such. They are mainly located on the right part of the face, which seems swollen. The nose appears fractured. Flows of blood, supposed to come from the pricks of the crown thorns, are visible on the face and the scalp.
The image such as it appears on the shroud: the body stands out in negative, the « bloodstains » in positive. If one converts in relief (opposite figure) the variations of color intensity, one obtains a low-relief
and not a body in 3D.
The photographic negative of the image reveals many details. The face seems swollen. But it is not deformed, whereas it should be if the shroud had really been applied to a human face.
The lesions of the body evoke flogging. The number of listed impacts is 100 to 120. Some light abrasions extend on a surface from 9 cm to 10 cm on the possible area of friction produced by the angle between the stipes (the vertical axis of the cross) and the patibulum (its horizontal axis). The knees are skinned.
A 4 cm by 1,5 cm wound is visible at the right side and has a size compatible with the point of the lancea at the time of the Romans, taking into account the post-mortem retraction of the fleshes. It is located at the level of the fifth intercostal space. A liquid resulting of this wound evokes a thick blood, running out vertically, modelled on the large indented muscle. It can correspond to an abundant flow of water and blood coming either from a pleural effusion, or from a pre-agony or post-traumatic hydro-pericardium (i.e. the presence of liquid in the membrane which surrounds the heart). A second flow of blood, posterior and transverse, could be explained by the horizontal position of the body after the Deposition and the draining of the lower vena cava containing the blood of the venous return.
In addition, the thorax is slack, the epigastria hollow is sagging, the abdomen is prominent, the quadricepses and glutei are salient, as many signs of the asphyxiation caused by the position of the inclined arms with an angle of 65° versus the stipes. Because at the time of a crucifixion, the rib cage cannot any more expand, oxygen rarefies, carbon dioxide and the lactates - products of the anaerobic metabolism - accumulate, causing a respiratory and metabolic acidosis and a tetanization of the muscles. In the beginning, the support on the feet makes it possible to rectify the body and facilitates the inspiration. But soon the respiratory distress and the cardio-circulatory failure occur leading to death. However, some doctors such Frederick Zugibe, think that the crucifixion does not cause asphyxiation (see page 124).
According to Dr. Veronique di Costanzo-Etienne of the hospital of Toulon (France), the characteristics of all these lesions correspond with anatomical requirements and are difficult to forge without medical knowledge. Such is not the opinion of Pr Claude Got, anatomo-pathologist and expert of the National Road Safety Council, for which this analysis is a mixture of description and interpretation. For him, the thought process is not restricted to describe the totality of the visible facts. It is connected with a search for explanation which tries, consciously or not to stick a posteriori to the passion of Christ. « The inaccuracy of the contour of these imprints does not enable me to advance a physio-pathological interpretation. Nothing in their form and their color says to me that these spots are of biological nature ». he concludes.
The image such as it appears on the shroud: the body stands out in negative, the « bloodstains » in positive. If one converts in relief (opposite figure) the variations of color intensity, one obtains a low-relief
and not a body in 3D.
The photographic negative of the image reveals many details. The face seems swollen. But it is not deformed, whereas it should be if the shroud had really been applied to a human face.
The lesions of the body evoke flogging. The number of listed impacts is 100 to 120. Some light abrasions extend on a surface from 9 cm to 10 cm on the possible area of friction produced by the angle between the stipes (the vertical axis of the cross) and the patibulum (its horizontal axis). The knees are skinned.
A 4 cm by 1,5 cm wound is visible at the right side and has a size compatible with the point of the lancea at the time of the Romans, taking into account the post-mortem retraction of the fleshes. It is located at the level of the fifth intercostal space. A liquid resulting of this wound evokes a thick blood, running out vertically, modelled on the large indented muscle. It can correspond to an abundant flow of water and blood coming either from a pleural effusion, or from a pre-agony or post-traumatic hydro-pericardium (i.e. the presence of liquid in the membrane which surrounds the heart). A second flow of blood, posterior and transverse, could be explained by the horizontal position of the body after the Deposition and the draining of the lower vena cava containing the blood of the venous return.
In addition, the thorax is slack, the epigastria hollow is sagging, the abdomen is prominent, the quadricepses and glutei are salient, as many signs of the asphyxiation caused by the position of the inclined arms with an angle of 65° versus the stipes. Because at the time of a crucifixion, the rib cage cannot any more expand, oxygen rarefies, carbon dioxide and the lactates - products of the anaerobic metabolism - accumulate, causing a respiratory and metabolic acidosis and a tetanization of the muscles. In the beginning, the support on the feet makes it possible to rectify the body and facilitates the inspiration. But soon the respiratory distress and the cardio-circulatory failure occur leading to death. However, some doctors such Frederick Zugibe, think that the crucifixion does not cause asphyxiation (see page 124).
According to Dr. Veronique di Costanzo-Etienne of the hospital of Toulon (France), the characteristics of all these lesions correspond with anatomical requirements and are difficult to forge without medical knowledge. Such is not the opinion of Pr Claude Got, anatomo-pathologist and expert of the National Road Safety Council, for which this analysis is a mixture of description and interpretation. For him, the thought process is not restricted to describe the totality of the visible facts. It is connected with a search for explanation which tries, consciously or not to stick a posteriori to the passion of Christ. « The inaccuracy of the contour of these imprints does not enable me to advance a physio-pathological interpretation. Nothing in their form and their color says to me that these spots are of biological nature ». he concludes.





